
Knee Osteoarthritis (OA) is characterized by progressive articular cartilage degeneration leading to debilitating pain and stiffness for millions worldwide. This condition commonly has a profound impact on the quality of life for patients leading to a slow decline in every-day activities. Historically, health providers have focused on symptomatic control and minimizing risk factors for OA. Conservative treatment often consists of corticosteroid (CSI) injections and nonsteroidal anti-inflammatory drugs (NSAIDs). Steroid injections, however, can be toxic to one’s cartilage. In addition, NSAIDs can have side effects on one’s gastrointestinal tract and kidneys. Platelet rich plasma (PRP) is an orthobiologic injection that has gained popularity in the treatment of knee arthritis recently.
PRP is acquired through the centrifugation of whole blood, resulting in a supraphysiologic concentration of platelets relative to whole blood. The delivery of PRP may stimulate an immunological and inflammatory response to supplement physiological healing by releasing growth factors and cytokines. In general, the composition of PRP can be further categorized into leukocyte-rich PRP (LR-PRP) preparations and leukocyte-poor PRP (LP-PRP) preparations. Activated platelets release alpha granules, which contain a plethora of growth factors including platelet-derived growth factor, transforming growth factor, insulin-like growth factor, fibroblast growth factor, and vascular endothelial growth factor. Overall, PRP is thought to decrease inflammation and modulate pain when injected into an arthritic joint. It can also increase blood flow and increase the strength of soft tissue
Recently, several systematic reviews and meta-analyses have been performed comparing PRP to corticosteroid and hyaluronic acid (HA) injections. In 2021 Heron et al. performed a systematic review including eight studies with over 640 patients and found that when compared to CSI injections, intra-articular PRP injections produce superior outcomes for symptomatic management of knee OA at 3, 6, and 9 months post-intervention. A more recent systematic review led by Singh et al. in 2022 showed PRP was more efficacious than HA in treating symptomatic knee OA compared to the placebo group. In a separate systematic review published in the American Journal of Sports Medicine Belk et al. reviewed 18 studies and found that LP-PRP may be a superior line of treatment for knee OA over LR-PRP but noted further studies are warranted to standardize leukocyte concentrations in PRP injections for treatment of knee OA. Recently, more attention has been directed at the platelet dosage of the PRP preparation and its effect on outcomes.
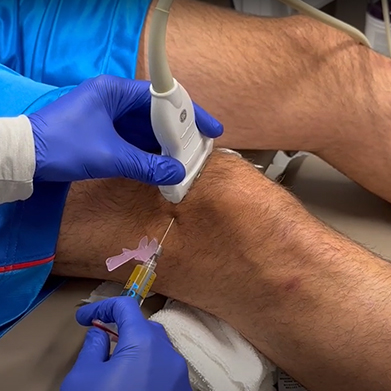
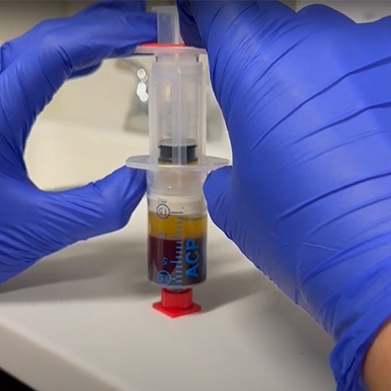
The process of obtaining a PRP injection is rather routine. One typically undergoes a blood draw from a peripheral vein. The blood is then spun down in a centrifuge. The plasma portion of the blood is separated (Figure 1) and then injected back into the joint of interest. We typically inject joints under ultrasound guidance to increase accuracy. Please see our video on a typical PRP injection.
In summary, PRP continues to demonstrate promise in the treatment of symptomatic OA and patients should discuss this treatment option with providers. The cost of PRP is quite variable depending on your geographic location. We published a recent study that demonstrated the cost of PRP often correlates to the mean income of residents in the area.
Please call and schedule an appointment with a board-certified sports medicine doctor to discuss PRP as a potential treatment option for you.